Improving Access to Care: Using Data to Understand the Relationships Between Hospitals and Hospices
All data used in this article was extracted from HealthPivots DataLab and is based on Medicare Fee-for-Service Claims released annually by CMS. In compliance with a DUA on file with CMS, patient counts less than 11 are not reported.
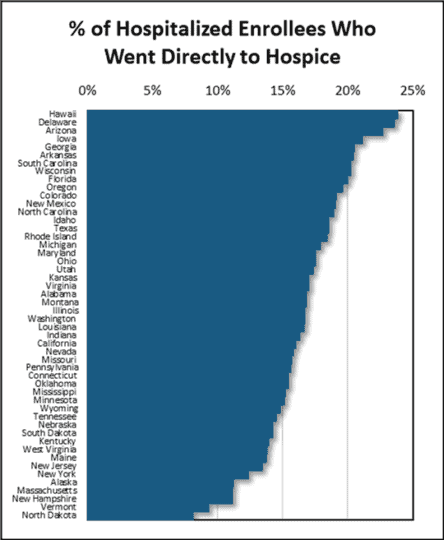
There is wide variability in timely access to hospice care after a hospitalization. Nationally in 2016, 17% of Medicare enrollees who died within six months of hospital discharge were discharged directly into hospice care. The highest performing state was Hawaii (23.8% of end-of-life patients referred directly to hospice) and the lowest performing state was North Dakota (8.1% of end-of-life patients referred directly to hospice). The figure below displays all states ranked for the percent of hospice eligible patients admitted directly to hospice.
Medicare Enrollees Discharged Directly to Hospice
Among Those Who Died Within Six Months of a Hospital Discharge
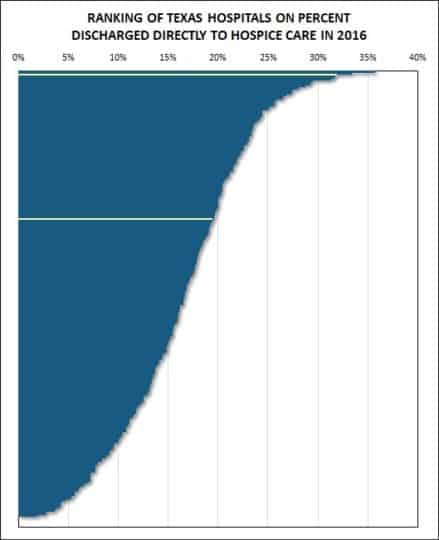
Examples of variations in referral patterns also appear within local communities. Drilling down to the level of individual hospitals at the local level provides a granular view of these differences in care patterns. Hospital referral patterns have a substantial impact on patients’ access to appropriate post-acute care. Within some communities, a patient’s care trajectory is significantly influenced by the hospital they are admitted to. Identifying hospitals that are missing opportunities to link patients with needed hospice care is an important step toward improving access.
Hendrick Medical Center and Shannon Medical Center in Texas are examples of two hospitals that are close geographically but with different post-acute care patterns. The post-acute discharge profiles below indicate a wide range in the post-acute use of hospice care.
Hospice Eligible Patients Admitted to Hospice from Example Hospitals

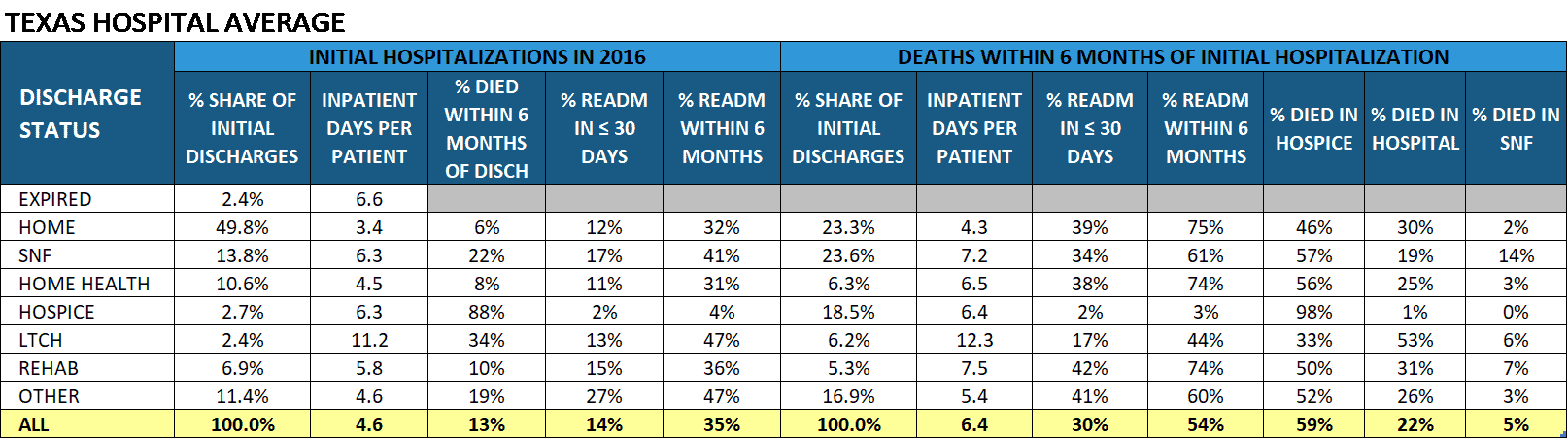
Among Medicare enrollees who were discharged live from a Texas hospital in 2016, 13.3% died within six months of their initial discharge. Of these enrollees –
- 5% were discharged directly to hospice care,
- 9% were admitted to hospice at a later date, and
- 6% died without receiving hospice care.
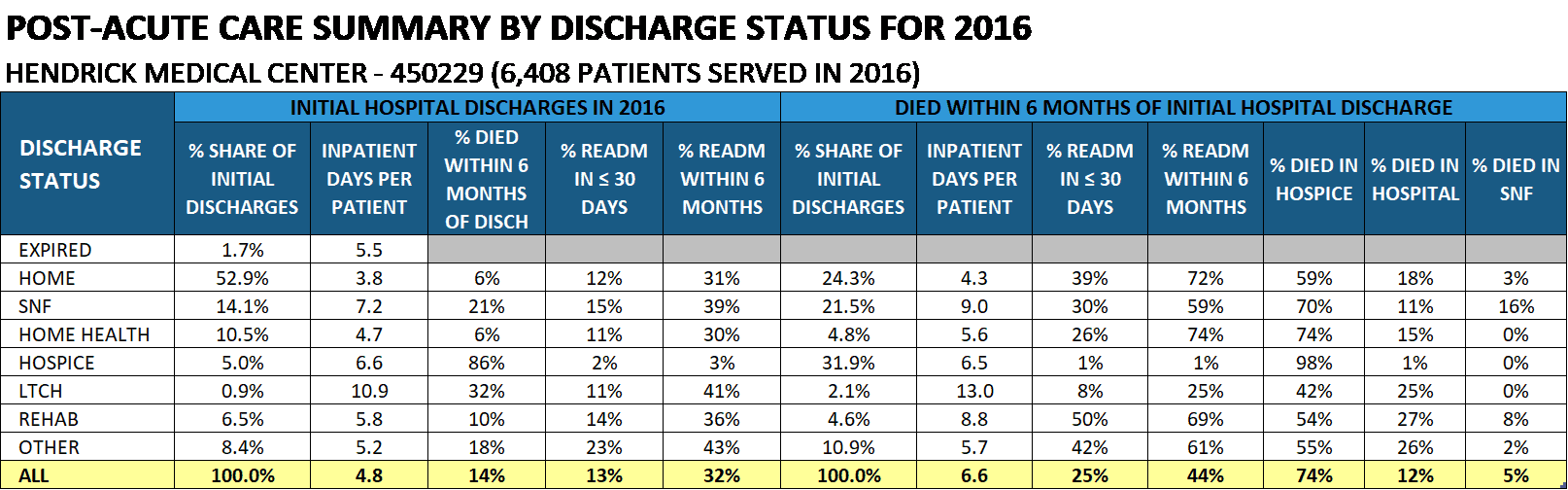
For Hendrick Medical Center Medicare patients, who died within six months of discharge –
- 9% were discharged directly to hospice care,
- 6% were admitted to hospice later, and
- 5% died without receiving hospice care.
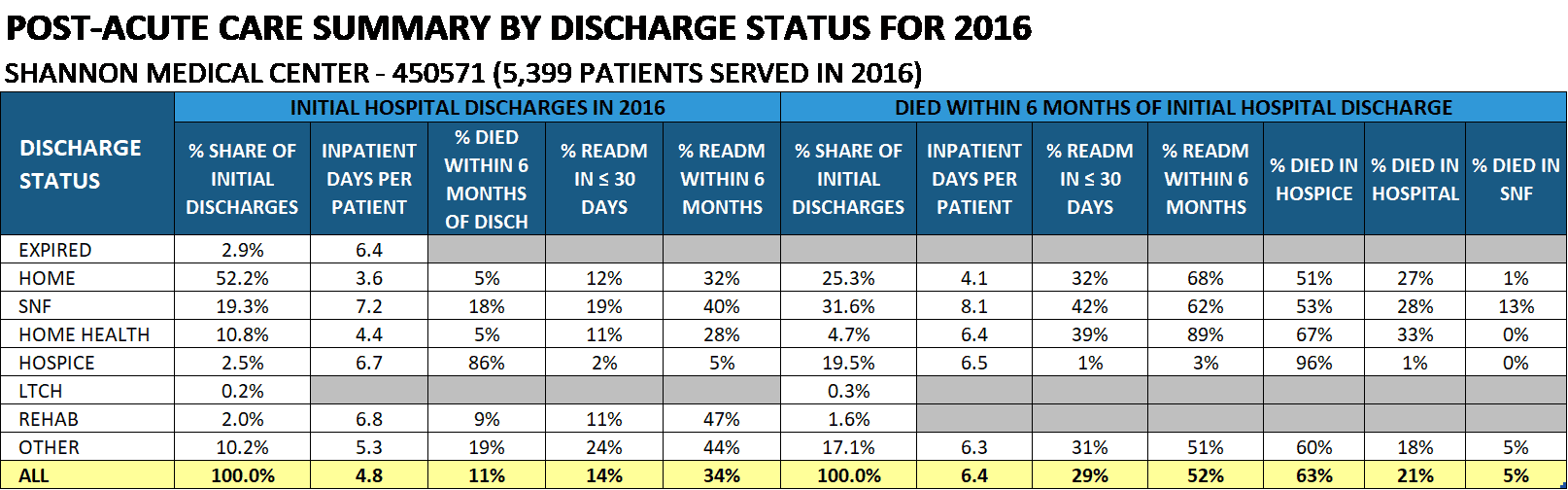
For Shannon Medical Center Medicare patients, who died within six months of discharge –
- 5% were discharged directly to hospice care,
- 2% were admitted to hospice later, and
- 3% died without receiving hospice care.
Both Hendrick Medical Center and Shannon Medical Center performed above the state averages for post-acute hospice use. However, patients discharged from Hendrick Medical Center received hospice care earlier. In fact, Hendrick Medical Center had the third highest rate of direct discharge to hospice among all Texas hospitals.

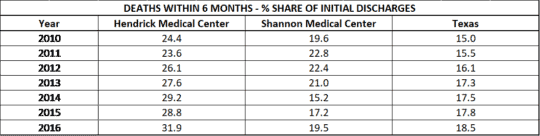
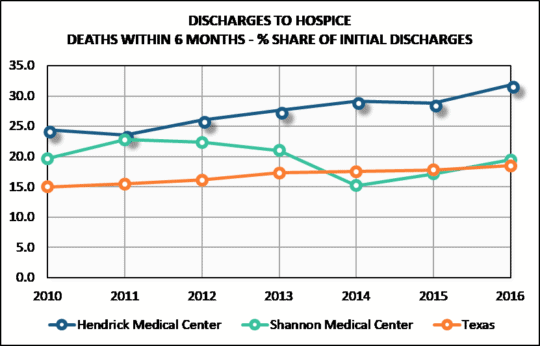
The trend in post-acute hospice use for these two hospitals paints a more complicated picture. Both hospitals outperformed the state rate in 2010 and in 2016. However, in 2010 the positions of the hospitals were reversed, with Shannon Medical Center discharging at a higher rate directly into hospice. As the state rate of post-acute hospice use slowly increased, Hendrick Medical Center made even more substantial gains while Shannon Medical Center’s rate declined.
A mismatch between a patient’s discharge plan and their post-acute care needs can result in unnecessary readmissions. For the state of Texas, the overall Medicare 30-day readmission rate was 14% in 2016. For enrollees who died within 6 months of hospital discharge, the 30-day readmission rate was much higher at 30%. In contrast, the 30-day readmission rate for enrollees discharged directly to hospice was much lower at only 2%. These data show that discharging more eligible patients directly to hospice care can reduce unnecessary hospital readmissions.
Shannon Medical Center had readmission rates slightly lower than the state averages, but Hendrick Medical Center had a substantially lower 30-day readmission rate (25% vs 30%) for enrollees who died within six months of hospital discharge. Higher rates of hospice care for end-of-life patients reduce hospital readmission rates.
Conclusions
End of life patients often have a pivotal hospital stay. Patients who are discharged directly to hospice care are much less likely to be readmitted to the hospital. Comparative data on discharge patterns at hospitals can identify opportunities for increased hospice use and reduced hospital readmissions.